
Manifesto
What is my purpose?
The moment that radicalized me was when I learned the following information:
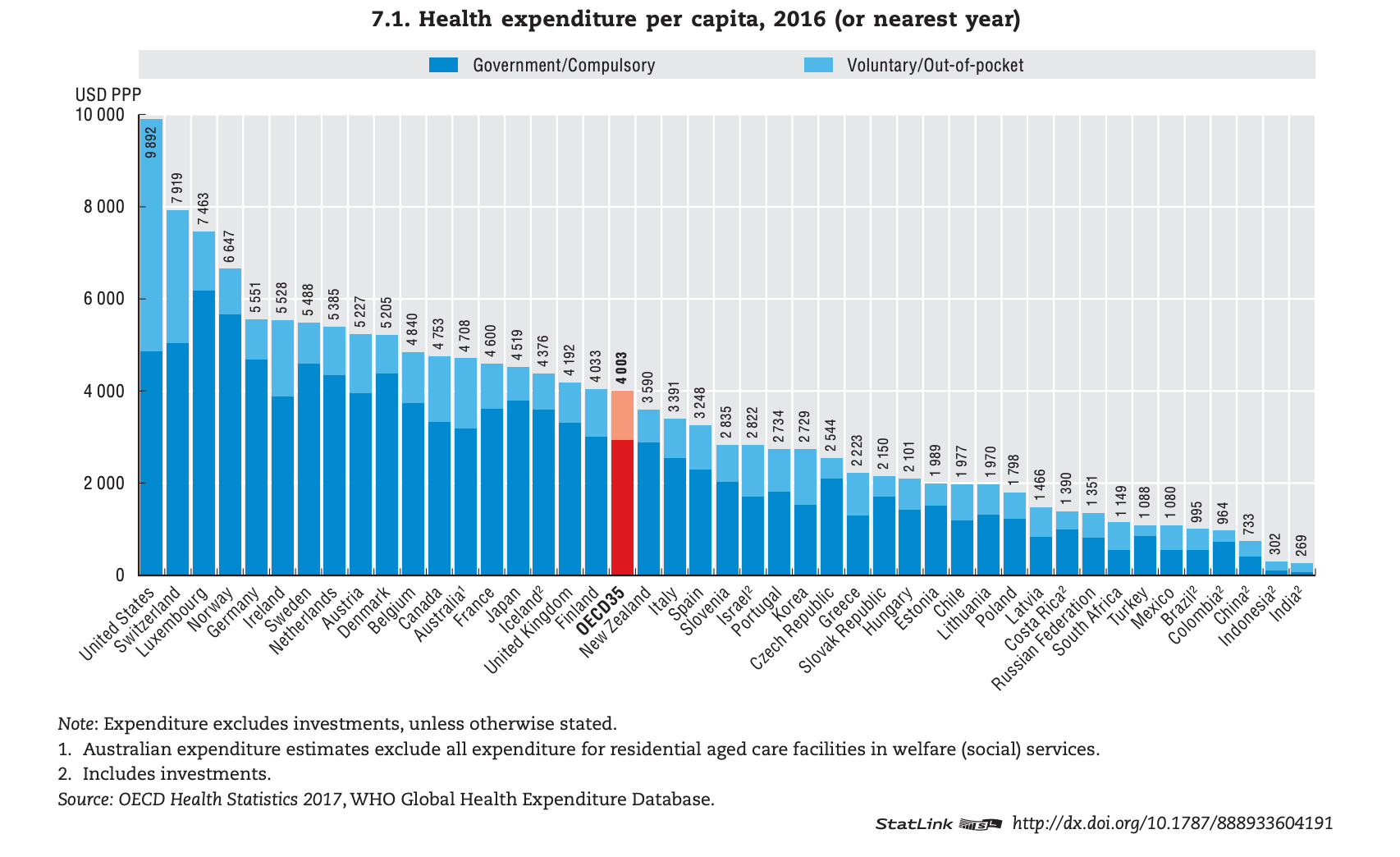
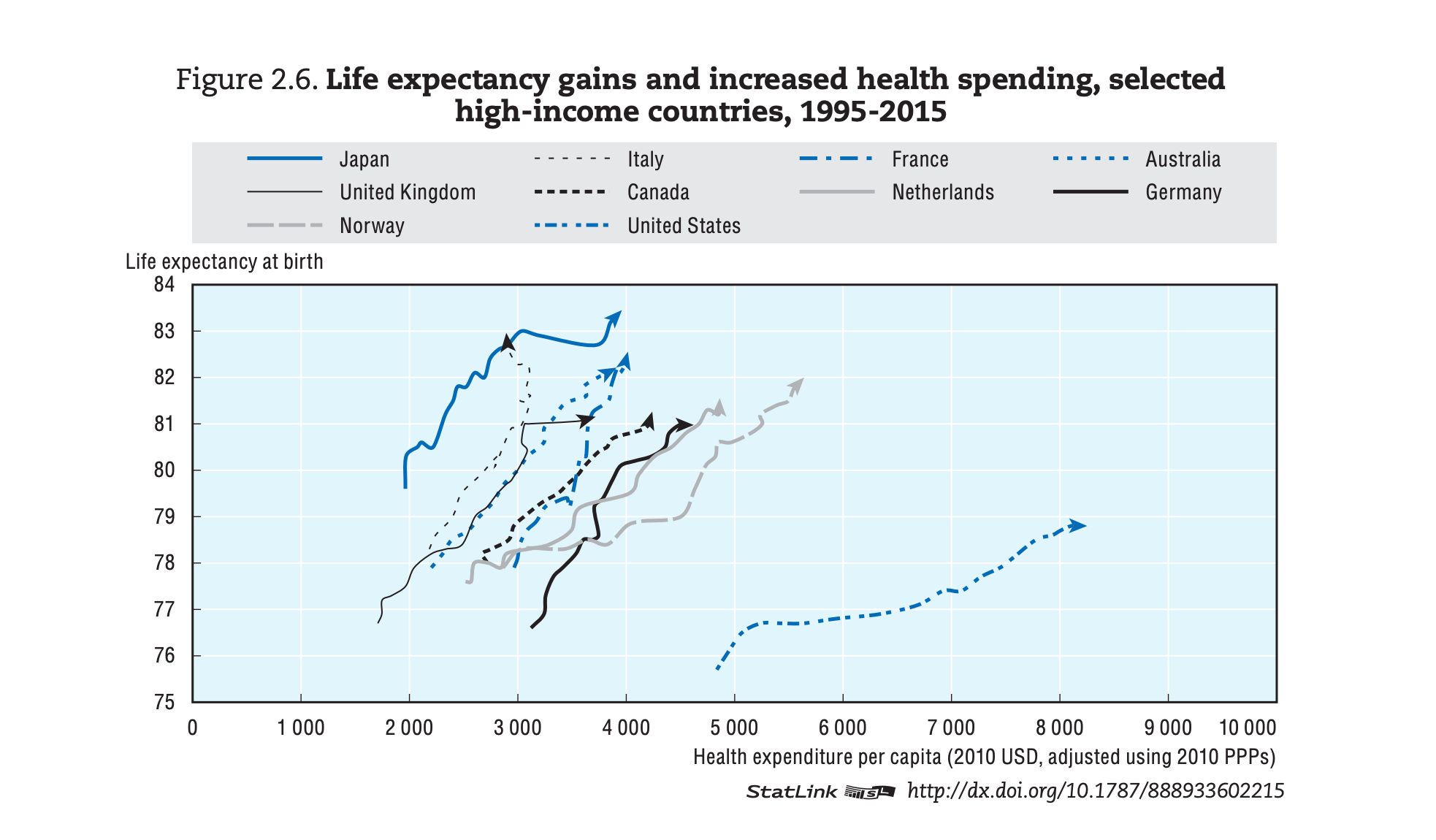
Looking at this graph, you might assume the United States has the world’s best healthcare system. After all, the U.S. spends nearly twice as much per citizen as the average country in the Organisation for Economic Co-operation and Development (OECD). However, the reality is starkly different:
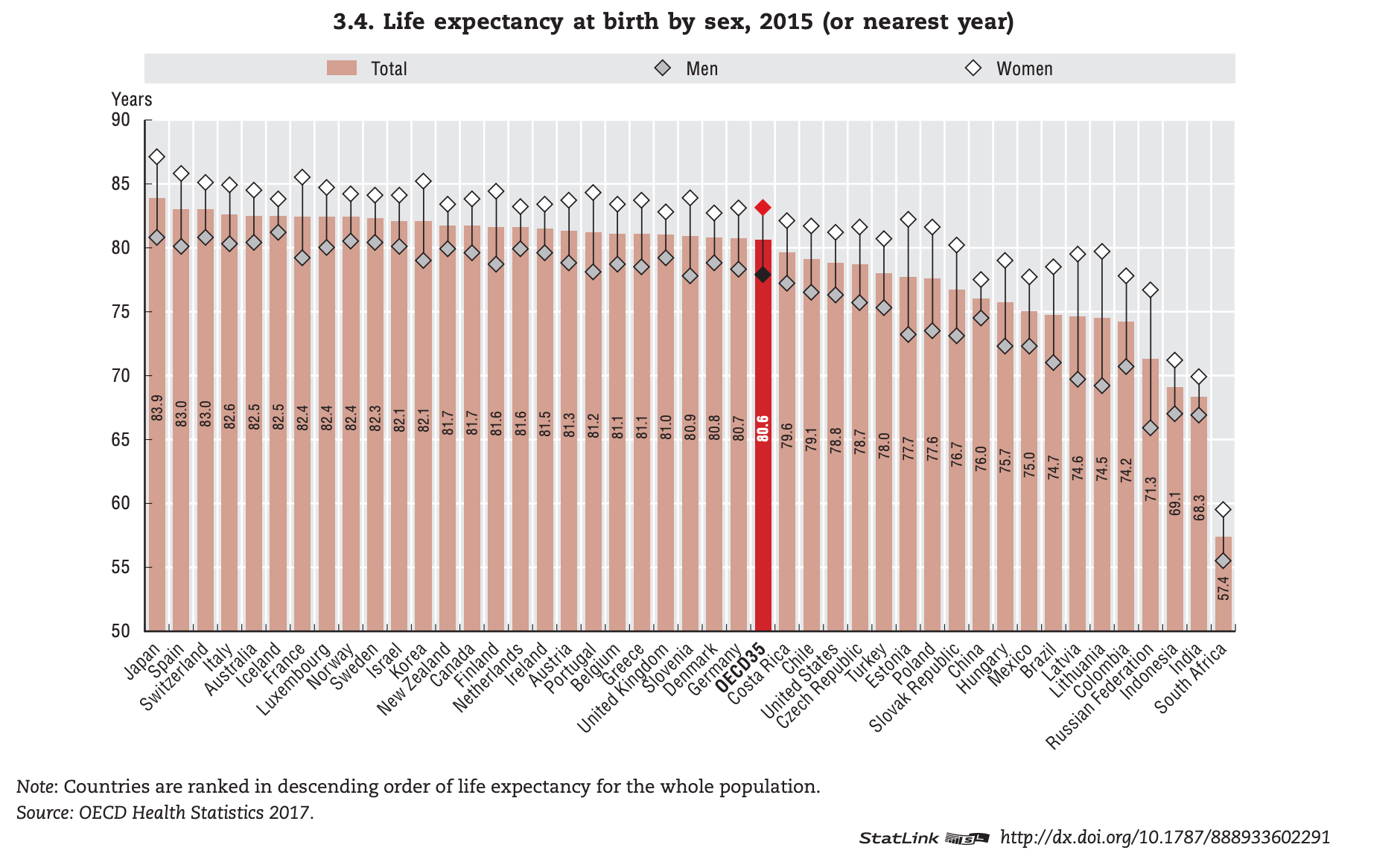
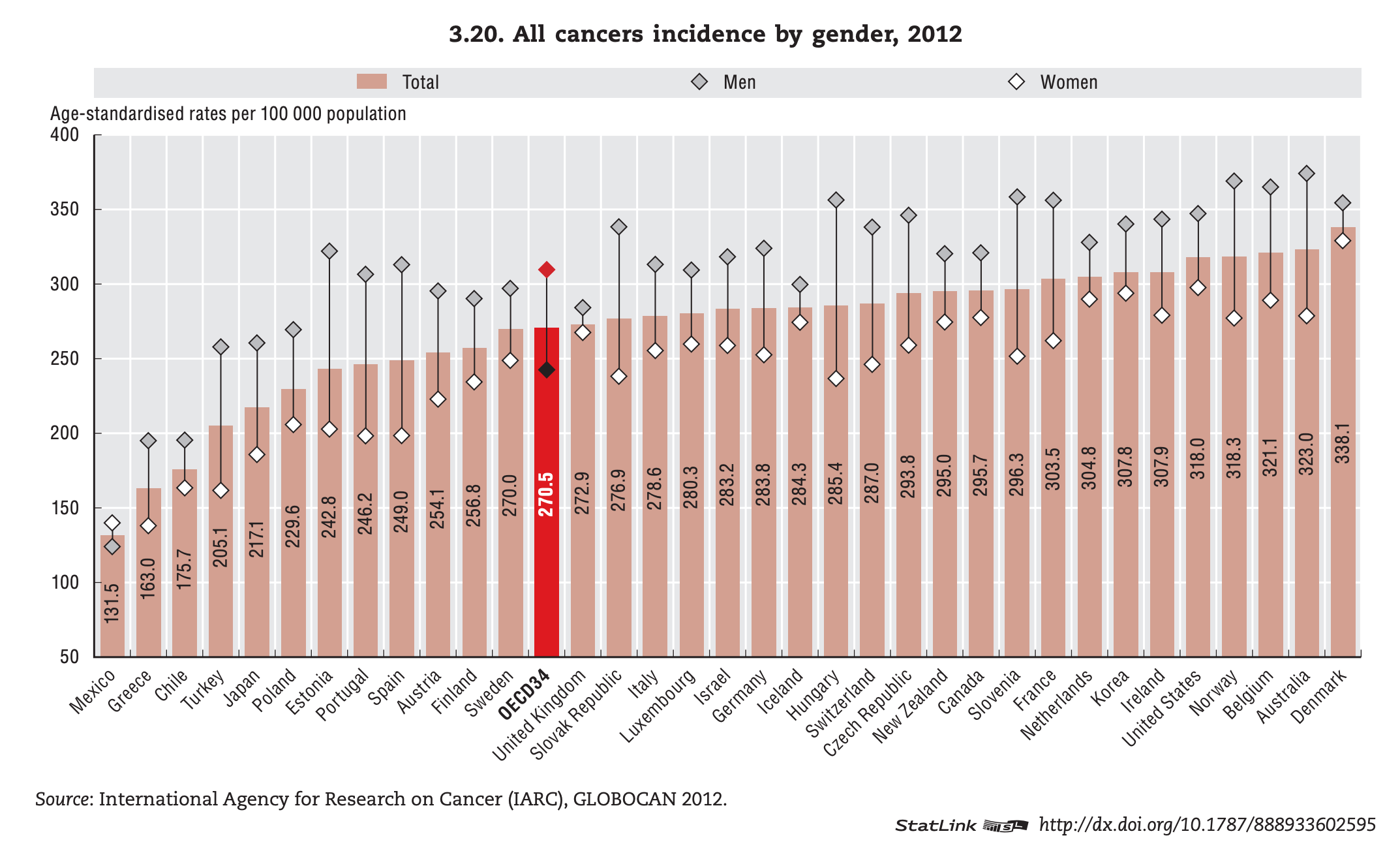
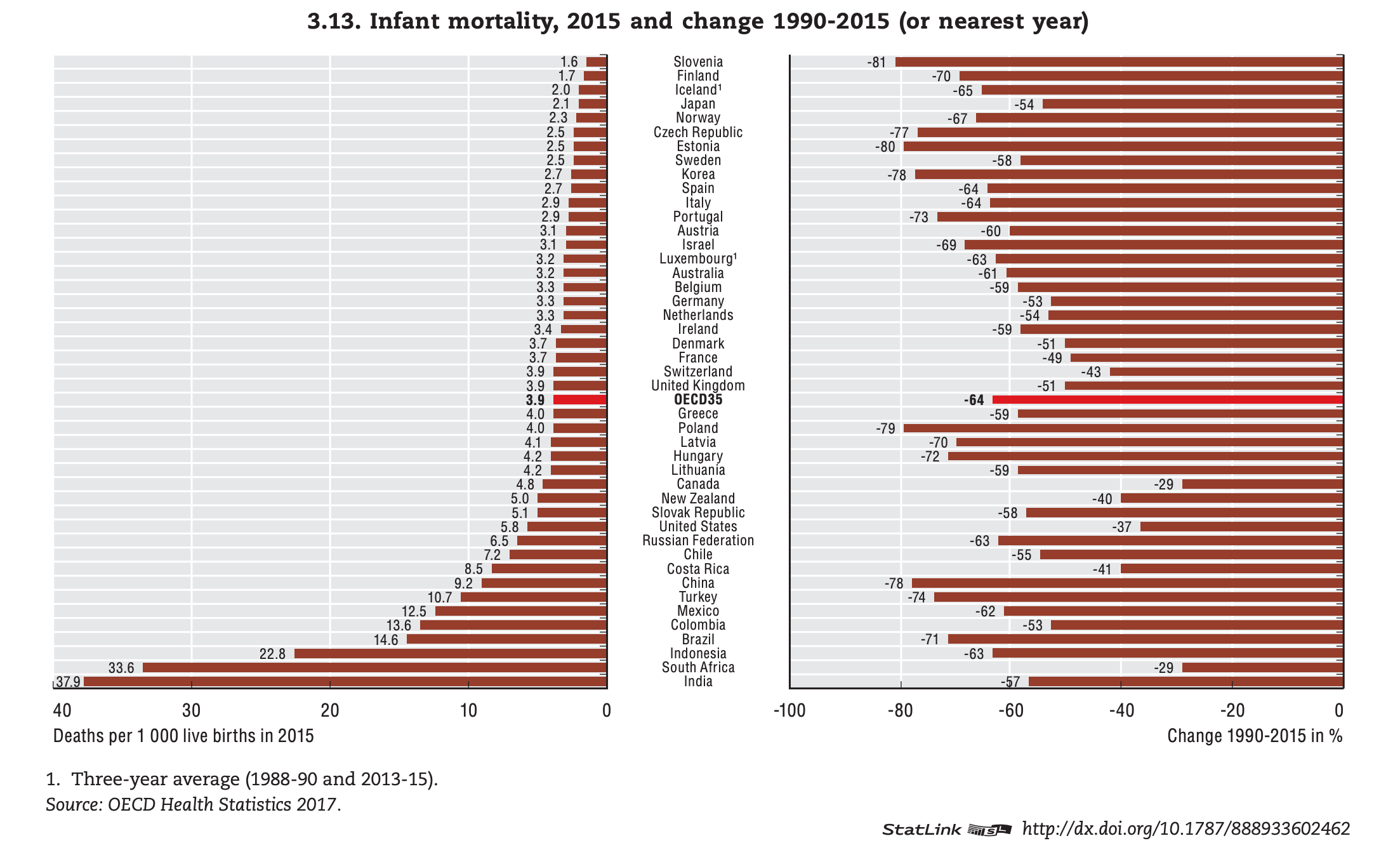
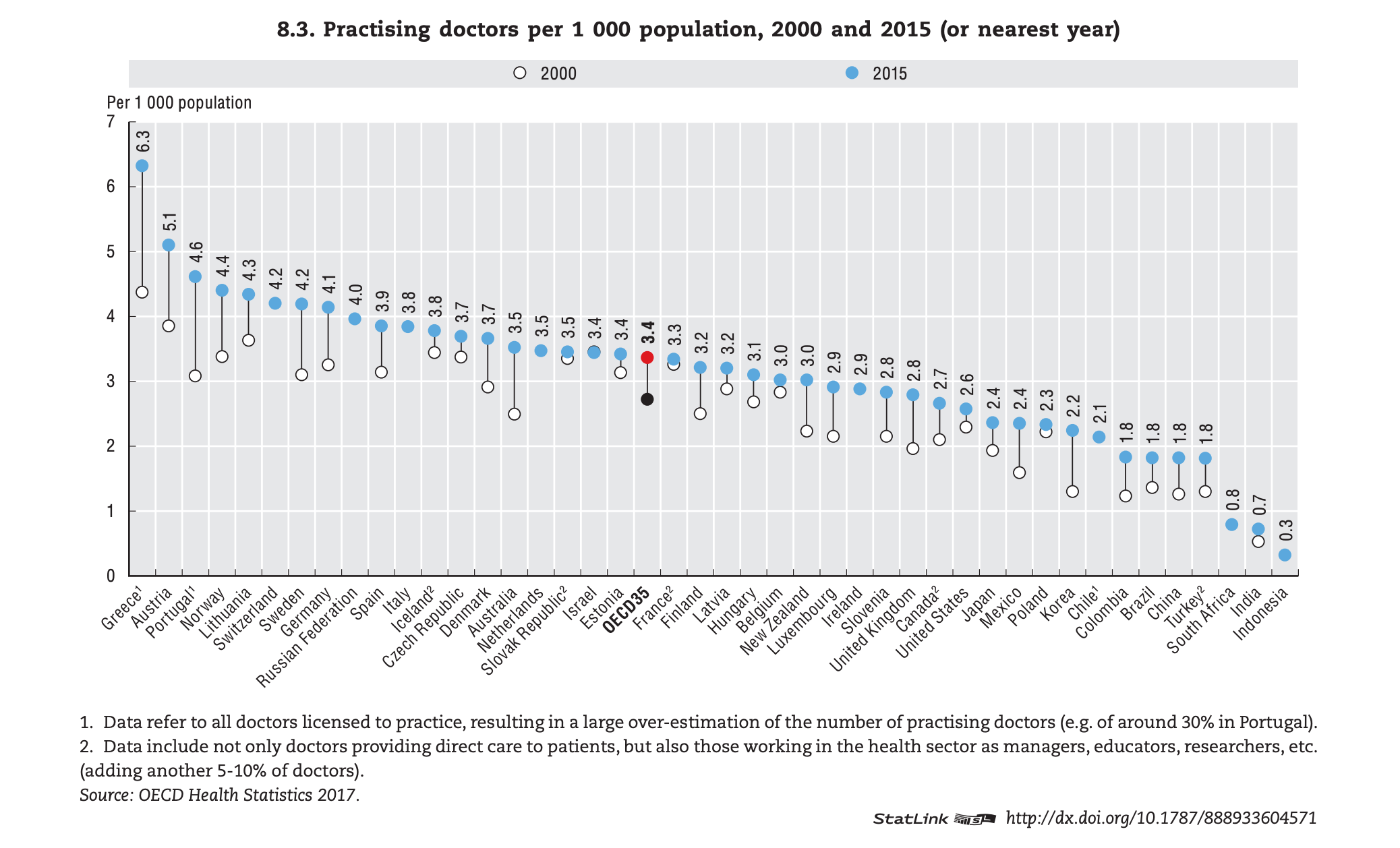
The United States doesn’t just fall short of being the best, it actually performs below average, and this is not just in life expectancy, but other metrics as well:
Plotted together, the U.S. is a clear outlier among high-income countries: paying more, getting less.
The cost of our inefficient system is that a great share of Americans skip care entirely because they can't afford it:
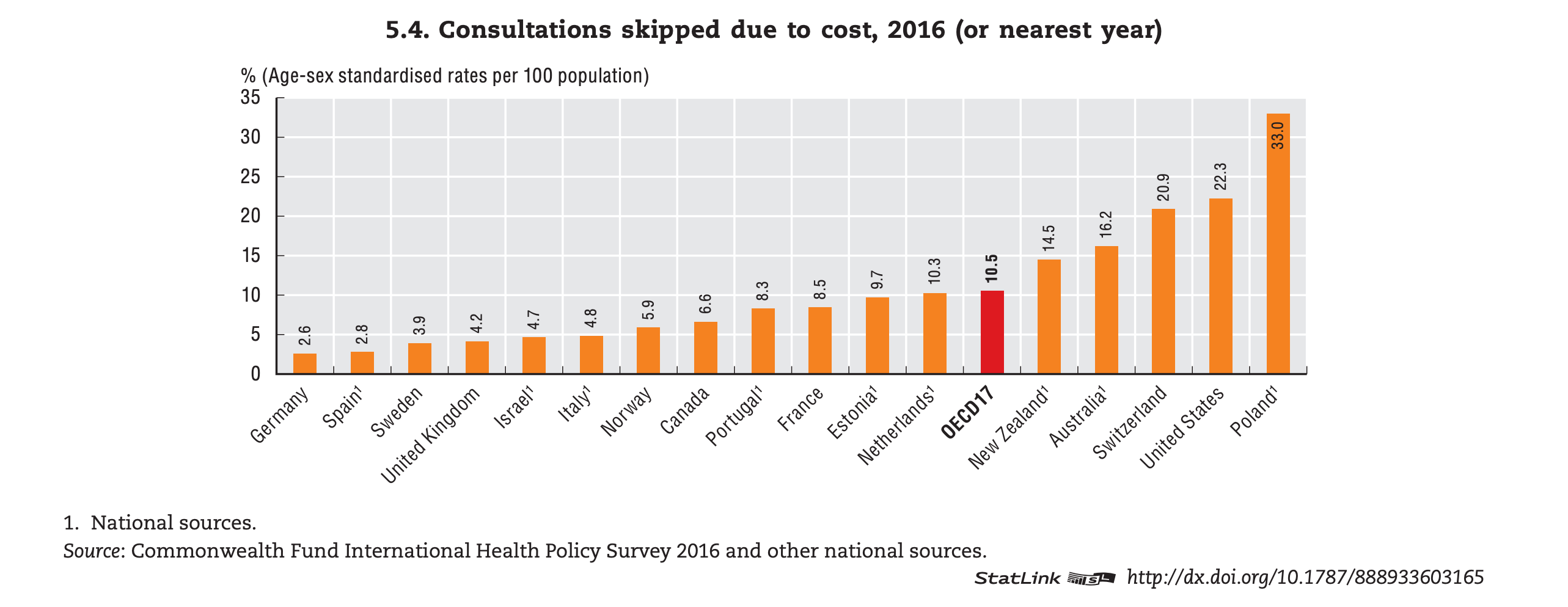
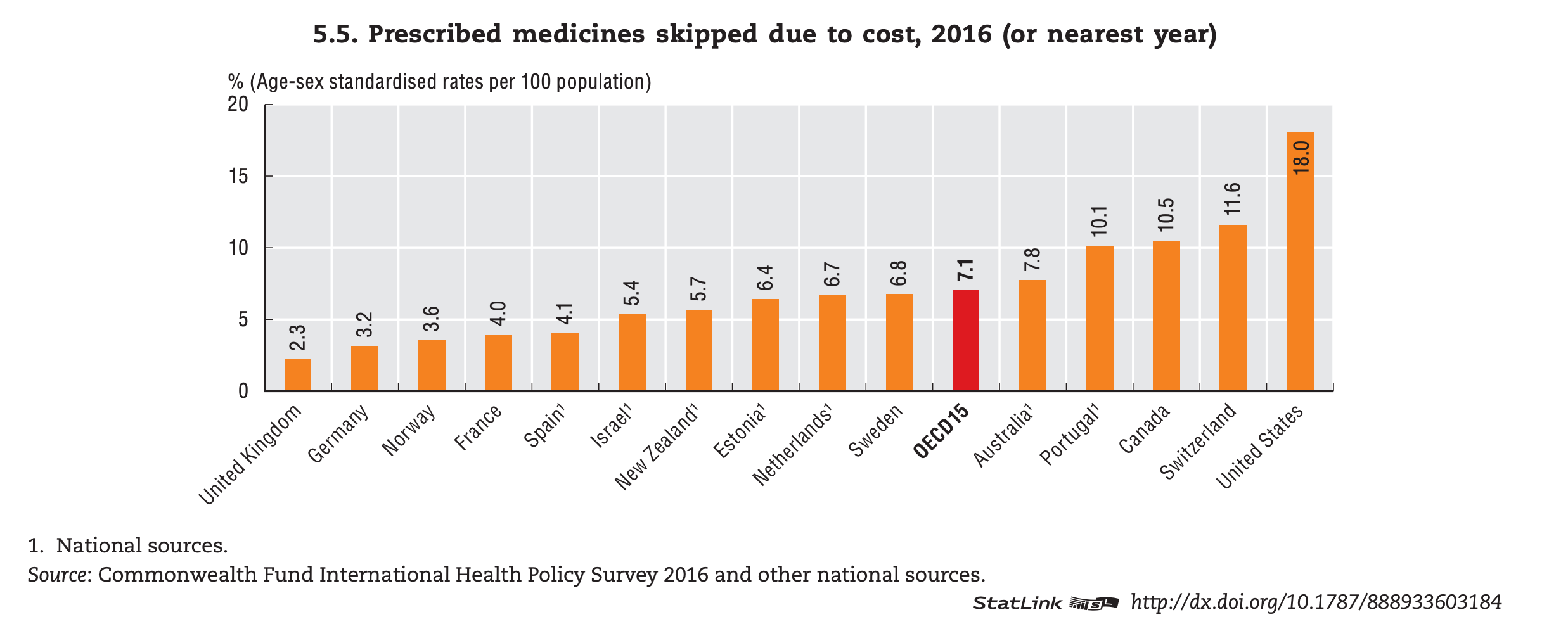
As you look at these figures, consider a time when you or a loved one deferred care because of the potential costs, only to face a much steeper physical and financial cost down the road. This issue is felt among the majority of us, regardless of race or ethnicity. This clip below illustrates that reality perfectly: a Trump voter explains why his encounter with affordable care in Japan radicalized his perspective.
The following video will only play for one minute.
I used to hope policy would fix this. I don't anymore, at least not within a timeframe that matters for the patients I'll see in residency. So I've started looking at the other lever this country actually pulls well: technology.
Here's where most clinicians stop reading, because "tech will fix healthcare" is what every founder with a pitch deck has been saying for years, but the cost curve hasn’t bent. I think I know why.
Health tech has been built by people who don't see patients, with clinicians brought in as advisors rather than founders. That arrangement lets companies check the "clinical input" box while still optimizing software for the people writing the checks: administrators, payers, investors. Clinicians don't need a louder seat at someone else's table. We need to build the table.
We are entering an era where clinical expertise matters more than coding proficiency. With AI handling the heavy lifting of initial development, frontline providers are now empowered to evolve from problem-spotters to prototype-builders and company founders.
Over the next four years I'll be building, writing, and documenting what it actually takes for a clinician to become a founder rather than a consultant: what works, what breaks, and what the people already doing this wish they'd known earlier. If I'm wrong, you'll watch me be wrong. If I'm right, you'll have a roadmap.
New post, biweekly on Wednesday mornings. Under 800 words. No filler.
If any of this resonates, subscribe and push back in the comments. I learn faster when you do.
Thank you for your time.
Best regards,
Pouya